

DRY EYE CONDITION
Meibomian Gland Dysfunction (MGD)
The most common cause of dry eye — and why drops alone won't fix it.
Meibomian gland dysfunction is responsible for up to 86% of all dry eye disease (Lemp et al., 2012). It happens when the oil glands in your eyelids become blocked or stop working, causing your tears to evaporate too quickly. If eye drops aren't giving you lasting relief, MGD is almost certainly the reason.
UNDERSTANDING MGD
What is meibomian gland dysfunction?
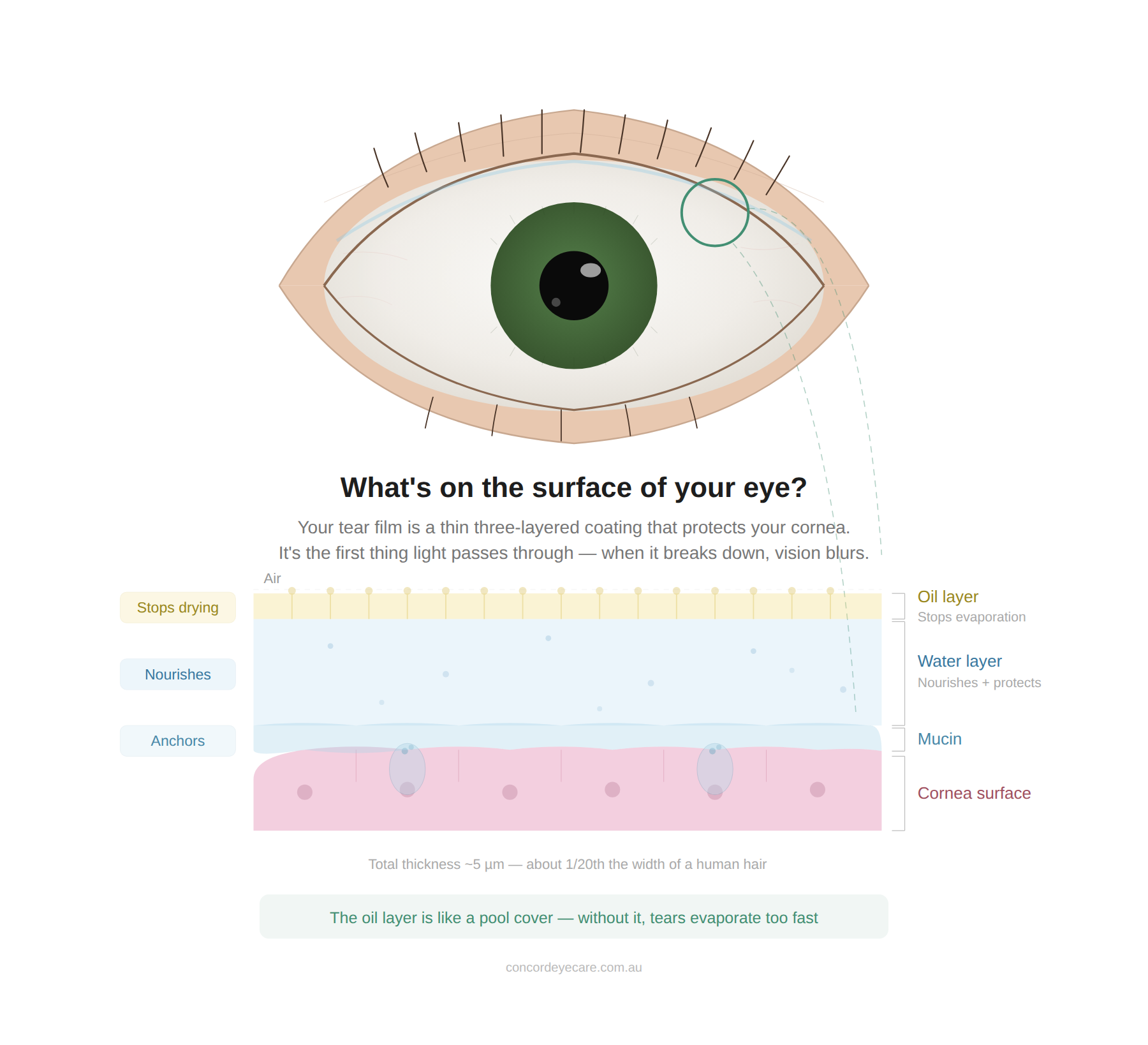
Meibomian gland dysfunction (MGD) is a chronic condition where the oil-producing glands in your eyelids become blocked, inflamed, or gradually waste away. These glands produce the oily outer layer of your tear film — the layer that stops your tears from evaporating. Without it, your eyes dry out within seconds of each blink.
MGD is remarkably common. Studies show it affects 39–50% of the general population depending on age group (Schaumberg et al., 2011), and it's present in up to 86% of people diagnosed with dry eye. Despite this, it's frequently missed because a standard eye test doesn't always include a detailed gland assessment.
The condition is progressive. Left untreated, blocked glands can permanently atrophy — they shrink and lose their ability to produce oil entirely. Once a gland is gone, it doesn't come back. That's why early diagnosis matters.

SYMPTOMS
What does MGD feel like?
MGD causes a persistent gritty or sandy feeling, burning that worsens through the day, tired eyes after screen use, blurry vision that briefly clears after blinking, and eyes that water excessively — your body's attempt to compensate for the missing oil layer. Most people don't connect these symptoms to their eyelids.
Symptoms typically worsen in air conditioning, heating, or wind — all of which accelerate tear evaporation when the oil barrier is compromised. If your eyes feel worse in these environments, that's a strong indicator of evaporative dry eye caused by MGD.
Here's the key clue: if lubricating drops help for a few minutes but the discomfort keeps coming back, the problem is likely oil deficiency, not water deficiency. Drops add moisture — but they can't replace the oil your meibomian glands should be producing.
THE REAL PROBLEM
Why eye drops aren't fixing your dry eye
Most over-the-counter dry eye drops supplement the watery layer of your tears. But if your dry eye is caused by MGD — which it is in 86% of cases — the underlying problem is oil deficiency, not water deficiency. You can add as much moisture as you like, but without the oil layer to seal it in, those tears evaporate within minutes.
Think of it like a pot of water boiling off. Adding more water doesn't help — you need the lid to stop the steam escaping. That "lid" is the oil your meibomian glands should be producing.
Drops aren't useless — lipid-based formulations can partially compensate. But drops alone can't unblock clogged glands, reverse inflammation, or prevent gland atrophy. For that, you need treatment directed at the glands themselves — like IPL therapy or targeted lid hygiene.
You may benefit from an MGD assessment if you...
Have been using eye drops for months without lasting improvement
Notice your eyes feel worse in air conditioning, heating, or wind
Experience burning, grittiness, or tired eyes that worsen through the day
Have been told you have "dry eye" but haven't had your meibomian glands specifically assessed
Your optometrist will assess your glands and tear film to determine the right approach.
Ready to find out what's actually causing your dry eye?
TYPES OF DRY EYE
MGD vs other types of dry eye
Dry eye has two main forms, and they need different treatment. Most people have MGD-related evaporative dry eye — but some have aqueous deficiency (reduced tear production), and many have a combination. A proper dry eye assessment distinguishes between them.
- Blocked or damaged meibomian glands
- Oil layer deficiency — tears evaporate too fast
- Worse in AC, wind, screen use
- Drops give temporary relief only
- Treated with IPL, warm compresses, lid hygiene
- Reduced tear production from lacrimal glands
- Water layer deficiency — not enough tears
- Often linked to autoimmune conditions (e.g., Sjögren's)
- Lubricating drops are a primary treatment
- May need prescription anti-inflammatory drops
This is why a proper assessment matters. If you're treating the wrong type of dry eye, drops will never be enough. We assess both components so we can target the actual cause.
WHAT TO EXPECT
How we diagnose meibomian gland dysfunction
A dry eye assessment at Concord Eyecare takes about 20 minutes and specifically evaluates your meibomian gland health. A standard eye test doesn't always check this — a dedicated assessment does. Here's what's involved:
We measure how quickly your tear film destabilises after a blink. A fast break-up time is a hallmark of evaporative dry eye.
We gently press on your eyelid glands to check whether they're producing clear, healthy oil or thick, blocked secretions.
Using a slit lamp microscope, we check your eyelid edges for inflammation, blocked gland openings, and structural changes.
We evaluate both the oil and water components to determine whether your dry eye is evaporative, aqueous-deficient, or a combination.
The diagnosis tells us exactly what's happening — which determines the treatment. No guesswork.
TREATMENT
How is meibomian gland dysfunction treated?
MGD treatment targets the glands directly — clearing blockages, reducing inflammation, and restoring healthy oil production. In our experience treating dry eye patients over 20 years, most people benefit from a combination approach tailored to their severity.
-
At-home management
Warm compresses (8–10 minutes daily with a heated eye mask), lid massage, and eyelid hygiene form the foundation. These need to be done consistently and with the right technique — we'll show you exactly how.
Browse lid hygiene products → -
Therapeutic eye drops
For moderate MGD with inflammation, prescription anti-inflammatory drops can help restore gland function. As therapeutically endorsed optometrists, we prescribe these directly — no GP referral needed.
-
IPL therapy (Intense Pulsed Light)
For moderate to severe MGD, IPL targets the root cause by reducing inflammation around the meibomian glands and improving oil flow. Research shows IPL improves dry eye symptoms in up to 87% of MGD patients (Craig et al., 2015).
How IPL works and what the evidence shows →
Your treatment plan is based on your specific assessment findings. We explain your options clearly and let you decide.
← Back to our full dry eye treatment overviewFREQUENTLY ASKED QUESTIONS
Your MGD questions answered
MGD is a chronic condition that can be effectively managed and controlled with the right treatment. Most patients notice significant improvement in comfort. However, once glands atrophy (waste away), that damage is permanent — which is why early treatment matters.
Common contributors include age, hormonal changes (particularly post-menopause), prolonged screen use (reduced blinking), contact lens wear, certain medications, and skin conditions like rosacea. It's usually a combination of factors.
They're closely related but not identical. Blepharitis is inflammation of the eyelid margin. MGD specifically refers to dysfunction of the oil glands within the eyelids. MGD is a leading cause of posterior blepharitis, and the two often occur together.
Most dry eye is caused by MGD — so if you have chronic symptoms, MGD is very likely involved. The only way to confirm is a dry eye assessment that specifically evaluates your meibomian gland function.
Your initial comprehensive eye examination is bulk billed through Medicare. If additional dry eye testing or IPL treatment is recommended, those are privately billed. We explain all costs upfront before any treatment begins.
Consistent at-home care (warm compresses and lid hygiene) typically shows improvement within 2–4 weeks. IPL therapy usually produces noticeable improvement within 3–4 sessions over approximately 3 months. We set realistic expectations during your assessment.
LEARN MORE
Related dry eye guides
- Lemp MA, et al. "Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort." Cornea. 2012;31(5):472-478.
- Nichols KK, et al. "The international workshop on meibomian gland dysfunction: executive summary." Invest Ophthalmol Vis Sci. 2011;52(4):1922-1929.
- Schaumberg DA, et al. "The international workshop on meibomian gland dysfunction: epidemiology and associated risk factors." Invest Ophthalmol Vis Sci. 2011;52(4):1994-2005.
- Craig JP, et al. "TFOS DEWS II Definition and Classification Report." Ocul Surf. 2017;15(3):276-283.
- Craig JP, et al. "Prospective trial of intense pulsed light for the treatment of meibomian gland dysfunction." Invest Ophthalmol Vis Sci. 2015;56(3):1965-1970.
- Jones L, et al. "TFOS DEWS II Management and Therapy Report." Ocul Surf. 2017;15(3):575-628.
- Optometry Australia. "Clinical Practice Guide for Dry Eye Disease." 2021.
BOOK AN ASSESSMENT
Find out what’s really causing your dry eye
A dry eye assessment takes about 20 minutes. We'll check your meibomian glands, evaluate your tear film, and give you a clear diagnosis — not a guess. No referral needed.