

Blepharitis · Concord Eyecare
Blepharitis is chronic — but with the right diagnosis and a treatment plan that fits your life, most patients get their comfort back. We'll help you get there.
Itchy, flaky, irritated eyelids?
Let's get you on top of it.

UNDERSTANDING BLEPHARITIS
What is Blepharitis?
Blepharitis is a chronic inflammation of the eyelid margins — the strip of skin where your lashes grow. It affects an estimated 37–47% of adults seen in primary eye care, making it one of the most common conditions we diagnose (Lemp & Nichols, 2009). It shows up as red, itchy, flaky lids that feel gritty or burn, especially first thing in the morning.
There are two types, and most patients have a mix of both. Anterior blepharitis affects the outside front edge of the lid where the lashes are — usually driven by Staphylococcal bacteria or Demodex mites. Posterior blepharitis affects the meibomian glands just behind the lash line, and it's the leading cause of evaporative dry eye worldwide (TFOS DEWS II, 2017).
In our experience at Concord Eyecare, blepharitis rarely comes alone — we commonly see it alongside dry eye, rosacea, or recurrent styes. It isn't something you cure once and forget. It's managed — a bit like eczema. Get on top of it, keep a daily routine, and symptoms stay quiet.
Anterior vs posterior blepharitis —
and how a stye differs
Anterior blepharitis affects the outside of the eyelid at the lash base and is usually driven by bacteria or Demodex mites. Posterior blepharitis affects the oil (meibomian) glands inside the lid and is the leading cause of evaporative dry eye. A stye, by contrast, is a single localised lump from one infected or blocked gland — not an inflammation of the whole lid margin.
- Crusting or flakes at lash base
- Red, itchy lid margins
- Collarettes = Demodex
- Often worse in the morning
- Burning, gritty, tired eyes
- Blurry vision that clears with blinking
- Leading cause of evaporative dry eye
- Often no visible flaking
- One tender spot, not whole lid
- Appears over 1–3 days
- Often resolves in 1–2 weeks
- Linked to underlying blepharitis
| Condition | Location | Main Cause | Key Sign |
|---|---|---|---|
| Anterior blepharitis | Outside lid edge at lash base | Staphylococcal bacteria or Demodex mites | Crusting, collarettes, morning flakes |
| Posterior blepharitis (MGD) | Inside lid — meibomian glands | Gland blockage, meibum stasis | Burning, gritty, evaporative dry eye |
| Stye (hordeolum) | Single lid location | Acute bacterial infection of a gland | Painful red lump, 1–3 day onset |
| Chalazion | Single lid location | Chronic blocked meibomian gland | Painless firm lump, slow resolution |
Symptoms of blepharitis — when to book an assessment
Common symptoms of blepharitis include red, itchy, or swollen eyelids, crusting or flakes at the base of the lashes, a burning or gritty sensation, and recurrent styes. Symptoms are typically worse in the morning and often flare with screen use. If any of these have been hanging around for more than a few weeks, it's worth booking an eye assessment.
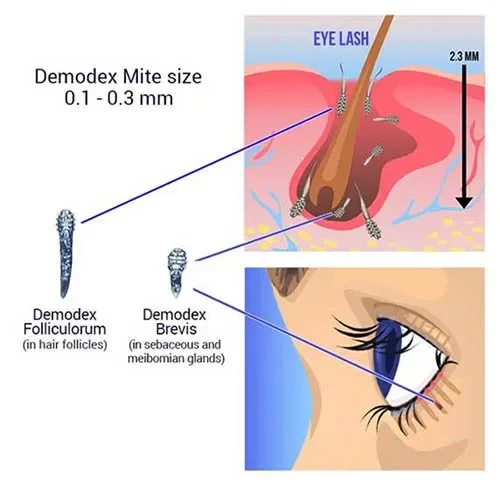
Demodex mites are present on most adult faces — but in some people, they overpopulate the lash follicles and cause chronic blepharitis. The telltale sign is collarettes: cylindrical dandruff clinging to the base of the lashes. If that's what we see on the slit lamp, the treatment plan shifts — we target the mites directly.
ROOT CAUSES
What causes blepharitis?
Blepharitis usually comes from one of three sources: bacteria, blocked oil glands, or Demodex mites — tiny parasites that live in your lash follicles. Research shows Demodex infestation is present in up to 75% of patients with chronic blepharitis (Liu et al., 2010), which is why diagnosis matters: the treatment changes depending on what's driving it.
Skin conditions like rosacea and seborrheic dermatitis raise your risk. So do hormonal changes, contact lens wear, makeup build-up, and long hours on screens — we blink less and the meibomian glands don't empty properly. In our practice we see the strongest link in patients over 50 and in contact lens wearers who skip their lid hygiene routine.
TREATMENT
How we treat blepharitis - from at-home care to in-clinic therapy
Blepharitis treatment works best as a stack, not a single fix. Most patients start with twice-daily warm compresses and lid hygiene wipes, add in Demodex-targeted cleansers if mites are present, and step up to prescription drops or IPL therapy when the condition is severe or persistent. In our experience, the patients who get the best long-term control are the ones who stick to a daily routine — not the ones chasing a one-off cure.
FREQUENTLY ASKED QUESTIONS
Your Blepharitis questions answered
Blepharitis is a chronic inflammation of the eyelid margins. It causes red, itchy, flaky lids and is usually driven by bacteria, blocked oil glands, or Demodex mites. It's one of the most common eye conditions we see in practice.
Not cured — but very well managed. Blepharitis is chronic, a bit like eczema or rosacea. In our practice, patients who follow a daily lid hygiene routine typically keep symptoms quiet long-term, with flare-ups only when the routine lapses.
No. Blepharitis isn't contagious — you can't catch it from someone else or pass it on. It's driven by your own skin bacteria, oil glands, or mites already present on most adult faces.
Blepharitis affects the whole lid margin — red, itchy, flaky. A stye is a single painful lump from one infected gland. Styes are often a complication of underlying blepharitis, which is why managing blepharitis reduces how often they come back.
Acute symptoms usually settle within 2–4 weeks of starting treatment. But because it's chronic, you'll keep a reduced daily routine to stop it coming back. Most patients do warm compresses and lid hygiene for life — like brushing your teeth.
Yes, with some care. During flare-ups, take a break from eye makeup and contacts to reduce irritation. Once controlled, you can return to both — just clean lids before applying makeup, remove it fully at night, and replace mascara every 3 months.
BOOK AN ASSESSMENT
Don't put up with itchy, irritated lids
Blepharitis gets worse the longer it's left. Book an assessment and we'll work out what's actually driving it — and build you a plan that fits your life.
LEARN MORE
Related reading
Blepharitis often overlaps with other eyelid and dry eye conditions. Here's where to learn more.
- Putnam CM. "Diagnosis and management of blepharitis: an optometrist's perspective." Clin Optom (Auckl). 2016;8:71-78. doi:10.2147/OPTO.S84795
- Lemp MA, Nichols KK. "Blepharitis in the United States 2009: a survey-based perspective on prevalence and treatment." Ocul Surf. 2009;7(2 Suppl):S1-S14.
- Liu J, Sheha H, Tseng SC. "Pathogenic role of Demodex mites in blepharitis." Curr Opin Allergy Clin Immunol. 2010;10(5):505-510. doi:10.1097/ACI.0b013e32833df9f4
- Trattler W, Karpecki P, Rapoport Y, et al. "The prevalence of Demodex blepharitis in US eye care clinic patients as determined by collarettes: a pathognomonic sign." Clin Ophthalmol. 2022;16:1153-1164. doi:10.2147/OPTH.S354692
- Fromstein SR, Harthan JS, Patel J, Opitz DL. "Demodex blepharitis: clinical perspectives." Clin Optom (Auckl). 2018;10:57-63. doi:10.2147/OPTO.S142708
- Huo Y, Mo Y, Wu Y, et al. "Efficacy of intense pulsed light therapy in treating ocular Demodex infestation." Cornea. 2024. [83% mite-free after 3 IPL sessions]
- Craig JP, Nichols KK, Akpek EK, et al. "TFOS DEWS II Definition and Classification Report." Ocul Surf. 2017;15(3):276-283. doi:10.1016/j.jtos.2017.05.008
- Nichols KK, et al. "The international workshop on meibomian gland dysfunction: executive summary." Invest Ophthalmol Vis Sci. 2011;52(4):1922-1929. doi:10.1167/iovs.10-6997a
- Lindsley K, Matsumura S, Hatef E, Akpek EK. "Interventions for chronic blepharitis." Cochrane Database Syst Rev. 2012;(5):CD005556. doi:10.1002/14651858.CD005556.pub2
- Navel V, Mulliez A, Benoist d'Azy C, et al. "Efficacy of treatments for Demodex blepharitis: a systematic review and meta-analysis." Ocul Surf. 2019;17(4):655-669. doi:10.1016/j.jtos.2019.06.004
- Optometry Australia. "Clinical Practice Guide for Dry Eye Disease." 2021.