
DRY EYE CLINIC · SYDNEY
Dry eye treatment Sydney
Most "dry eye" isn't actually dryness. About 86% of cases are evaporation from blocked oil glands — drops don't fix it. We diagnose the type first, then treat the cause.
Reviewed by Dr Nikki Peng · Last updated May 2026
WHAT IS DRY EYE
Why are there three types of dry eye?
Most "dry eye" isn't actually dry
Most people reach for over-the-counter drops, assuming "dry eye" means their eyes don't make enough tears. For the majority of patients, that's the wrong answer — their eyes are making tears. The oil layer that should be slowing evaporation has broken down, and the tears are evaporating before they can do their job. Drops alone don't repair the oil glands.
| Feature | Evaporative dry eye | Aqueous-deficient | Mixed dry eye |
|---|---|---|---|
| Mechanism | Tear film evaporates too fast due to oil-layer deficiency | Lacrimal glands produce insufficient tear fluid | Both mechanisms together |
| Prevalence | ~86% of cases (Lemp 2012) | ~10% of cases | Common in long-standing disease |
| Common causes | Meibomian gland dysfunction, blepharitis, demodex, ageing | Sjögren's syndrome, autoimmune disease, some medications | Often what untreated evaporative disease becomes |
| Key diagnostic test | Meibography + NIBUT | Schirmer's test + osmolarity | Full diagnostic panel |
| First-line treatment | Lid hygiene, warm compresses, IPL therapy | Tear supplementation, punctal plugs | Combination — lid-focused + tear supplementation |
SYMPTOMS
Do these chronic symptoms sound familiar?
Common signs of dry eye disease
The assessment below uses the international TFOS DEWS II diagnostic criteria. Tick the symptoms you experience regularly to get an indicative symptom burden score — useful context to bring to your dry eye assessment.
Educational symptom check — not a diagnosis. This gives you a sense of your symptom burden. Only a clinical assessment can identify what's actually causing your symptoms and what will help.
Dry Eye Symptom Check
Informed by the symptom areas used in the TFOS DEWS II framework. Tick the symptoms you notice regularly to see your symptom burden.
Awaiting your answers…
Tick the symptoms above to see your symptom burden.
If you're ticking several of these, it's worth getting a proper assessment. Dry eye is a chronic condition — it doesn't go away on its own, and it tends to get worse if the underlying cause isn't treated.
HOW WE DIAGNOSE
How do you diagnose the type of dry eye?
Finding out why your eyes are dry
Standard eye tests don't usually look closely at the tear film or the oil glands. A proper dry eye work-up needs different equipment and a different conversation — symptom patterns, screen use, medications, contact lens history, hormonal changes — backed up by diagnostic imaging.
Non-invasive tear break-up time (NIBUT)
The Medmont E300 projects a pattern onto your tear film and measures how long it stays stable. No fluorescein dye, no stopwatch. Tells us whether your tear film is breaking down too fast — the hallmark of evaporative dry eye.
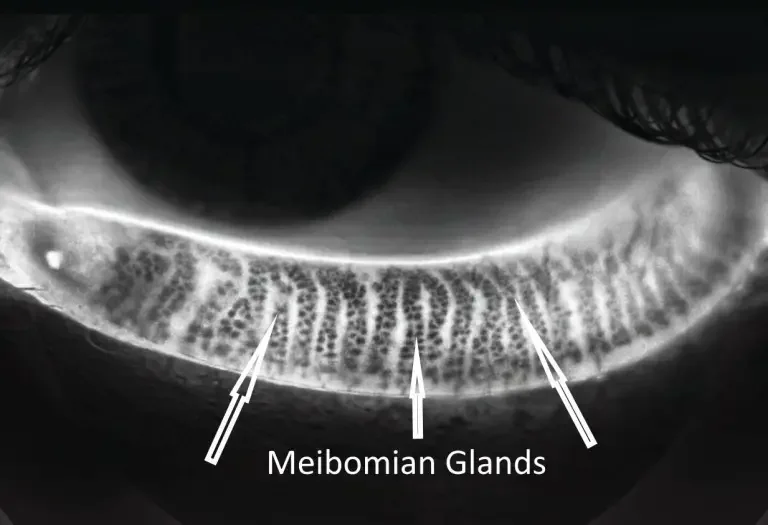
Meibography
The Meibovue meibographer images the oil glands in your eyelids. Healthy glands are long and intact. Damaged or atrophied glands look shortened or absent. This is structural information — it tells us how much gland function we're working with.
Schirmer's test (when indicated)
For suspected aqueous-deficient dry eye, the Schirmer's test measures actual tear production volume over five minutes. Used selectively — not every patient needs it, but it's diagnostic gold standard for ruling in or out aqueous deficiency.
Tear film and lid assessment
Slit-lamp examination of the lid margins, lash base, and meibomian gland openings. Helps us identify blepharitis, demodex, and gland blockages that drive evaporative dry eye.
If you'd like the diagnostic work-up without committing to a full treatment programme, our $50 Dry Eye Test Package covers NIBUT and meibography only — useful if you want to know what's going on before deciding on next steps.

IPL TREATMENT
Treating the root cause, not just the symptoms
Medical-grade IPL for evaporative dry eye
For moderate to severe meibomian gland dysfunction and evaporative dry eye, IPL (Intense Pulsed Light) targets the underlying inflammation rather than just managing symptoms. We use the E-Eye device — one of the few medical-grade IPL systems designed specifically for dry eye. Our all-inclusive programme covers the suitability assessment, four treatment sessions, and all follow-up reviews.
Ready to find out what's actually going on?
WHY CONCORD EYECARE
Dry eye is a spectrum. We treat it as one.
Diagnosis-first, treatment second — always
We work out the type first
Evaporative, aqueous-deficient, or mixed — the right treatment depends on which one you have. A proper diagnosis is why IPL works for the right patients, and why we don't recommend it for the wrong ones.
Equipment most optometrists don't have
Meibography and non-invasive tear break-up time aren't part of a standard eye test — they're dedicated dry eye diagnostics that need dedicated equipment. We have both: the Meibovue meibographer and the Medmont E300.
Everything under one roof
All three optometrists are therapeutically endorsed. If you need prescription drops or medication alongside lid therapy or IPL, we prescribe directly — no GP visit, no delays, one clinical file.
COMMON QUESTIONS
Dry eye — your questions answered
Six questions we hear from patients every week
What causes dry eye?
Most dry eye is caused by meibomian gland dysfunction — the oil glands in your eyelids stop producing enough quality oil, and your tear film evaporates too quickly. The international TFOS DEWS II Report (2017) puts evaporative disease at roughly 86% of cases. Other causes: age-related tear gland decline, autoimmune conditions like Sjögren's syndrome, prolonged screen use, contact lens overwear, and certain medications. The first step is identifying which mechanism applies to you.
Can dry eye be cured?
Dry eye is generally a chronic condition rather than something that's cured outright — but it can be well controlled. With the right diagnosis and a treatment plan that addresses the underlying cause (not just the symptoms), most patients experience meaningful, lasting improvement. The goal is symptom control and protection of the meibomian glands you still have.
How do you diagnose dry eye?
A proper diagnosis combines a detailed history with diagnostic imaging — non-invasive tear break-up time (NIBUT), meibography, slit-lamp examination of the lids and tear film, and Schirmer's test where aqueous deficiency is suspected. These tests aren't part of a standard eye test and need dedicated equipment. They tell us which subtype of dry eye you have so we can recommend the right treatment.
Is dry eye treatment covered by Medicare?
The diagnostic consultation is generally covered by Medicare when bulk-billed. Some treatments — including IPL and dedicated dry eye assessments using specialised equipment — are not Medicare-eligible. We're upfront about which parts of your treatment are bulk-billed and which carry a fee, before you commit to anything.
Do I need a GP referral?
No. You can book a dry eye assessment directly with us — no GP referral required. All three of our optometrists are therapeutically endorsed, which means we can prescribe medication for dry eye where appropriate, without sending you back to the GP first.
What's the difference between evaporative and aqueous-deficient dry eye?
Evaporative dry eye (about 86% of cases) happens when the oil layer of your tears breaks down and tears evaporate too quickly — usually from meibomian gland dysfunction. Aqueous-deficient dry eye (about 10%) happens when the lacrimal glands don't produce enough fluid — often related to autoimmune disease like Sjögren's syndrome. The treatment pathway is different for each — diagnosis decides direction.
PATIENT REVIEW
What a dry eye patient said
Real experience from a Sydney patient
"Mark treated my dry eyes with IPL and I can't thank him enough. I've been suffering with dryness for the past few years and my eyes use to look red, sore and tired no matter how many times I put lubricating drops in. After my 3rd session of IPL, I noticed an improvement and by the 4th session, the dryness was almost completely gone. I'm so happy! Now I can sit in front of the computer and be in an air conditioning room without feeling any irritation or blinking every second. An added bonus is my right eye (the eye that suffered with more dryness) use to be more droopy than my left eye but since the treatment, they're symmetrical, yay! Not sure if it was a coincidence but either way I'm really happy with the results and service. Thanks again Mark!"
CLINICAL REFERENCES
Peer-reviewed sources cited on this page
- Craig JP, Nichols KK, Akpek EK, et al. (2017). TFOS DEWS II Definition and Classification Report. The Ocular Surface, 15(3):276–283.
- Wolffsohn JS, Arita R, Chalmers R, et al. (2017). TFOS DEWS II Diagnostic Methodology Report. The Ocular Surface, 15(3):539–574.
- Jones L, Downie LE, Korb D, et al. (2017). TFOS DEWS II Management and Therapy Report. The Ocular Surface, 15(3):575–628.
- Stapleton F, Alves M, Bunya VY, et al. (2017). TFOS DEWS II Epidemiology Report. The Ocular Surface, 15(3):334–365.
- Lemp MA, Crews LA, Bron AJ, Foulks GN, Sullivan BD. (2012). Distribution of aqueous-deficient and evaporative dry eye in a clinic-based patient cohort. Cornea, 31(5):472–478.
- Nichols KK, Foulks GN, Bron AJ, et al. (2011). The International Workshop on Meibomian Gland Dysfunction: Executive Summary. Investigative Ophthalmology & Visual Science, 52(4):1922–1929.
- Toyos R, McGill W, Briscoe D. (2015). Intense pulsed light treatment for dry eye disease due to meibomian gland dysfunction. Photomedicine and Laser Surgery, 33(1):41–46.
Serving Sydney families and individuals with chronic dry eye. Concord Eyecare is located at 161 Concord Road, North Strathfield. Patients travel from across the Inner West and Greater Sydney — including Concord, Drummoyne, Abbotsford, Burwood, Five Dock, Strathfield, Homebush, Rhodes, Mosman, Lane Cove, and the Hills district — for dedicated dry eye assessment and IPL therapy.
READY WHEN YOU ARE
Your eyes don't have to feel like this forever
No GP referral needed. All three optometrists are therapeutically endorsed. Bookings Monday to Saturday.